

What Trauma-Informed Language Looks Like in Session Notes
A note written in five minutes between sessions gets read ten years later by a provider who never met the client. Under OASAS Part 822, that’s how long the record stays on file. The words you choose today are the client’s history tomorrow.
This is the case for trauma-informed documentation language. Not as a courtesy. As the thing that decides what the next reader believes about this person. What Trauma-Informed Care Actually Requires in an OASAS-Certified Setting names two examples of this. Here’s the rest of the picture.
Let’s jump in and see why clinical language in session notes outlasts the room it was written in, a language swap list you can use today, trauma-informed progress notes examples across four note types, and a one-sentence test for catching the gap between what you saw and what you assumed.
Why Word Choice in Notes Outlasts the Session
A session note doesn’t stay between you and the client. It is reviewed during utilization review, read by the future treatment team after a transfer, and retained for years under OASAS recordkeeping rules. Stigmatizing language in documentation travels with the chart every time.
Research backs this up directly. A 2018 study in the Journal of General Internal Medicine gave physicians-in-training one of two identical patient charts. One used neutral language. The other used stigmatizing language, like describing a patient as drug-seeking. Even readers who recognized the bias still treated the patient’s pain less aggressively afterward. The words moved the care.
Clinical language in session notes is intended to inform care rather than to deliver a verdict. Accurate, trauma-informed documentation avoids euphemism and avoids pathologizing the individual while clearly describing behaviors. Emphasizing collaborative documentation fosters transparency and encourages shared understanding among providers and clients. This approach facilitates better client engagement and promotes more personalized care. Trauma-informed language serves as the only reliable safeguard against drifting into stigmatizing or imprecise descriptions.
What this means for documentation:
- A note outlives the session it describes
- Bias in a chart transfers to the next clinician who reads it
- Stigmatizing language in documentation changes care decisions you’ll never see
Trauma-informed documentation language isn’t about softening the truth. It’s about making sure the truth survives the handoff intact.
The Language Swap List
Most stigmatizing language in documentation isn’t intentional. It’s shorthand, written fast, between clients. The fix is a swap, not a rewrite. Clinical language in session notes should describe behavior, not character. Collaborative Documentation That Actually Helps Substance Use Counselors and Clients covers the workflow this swap builds on.
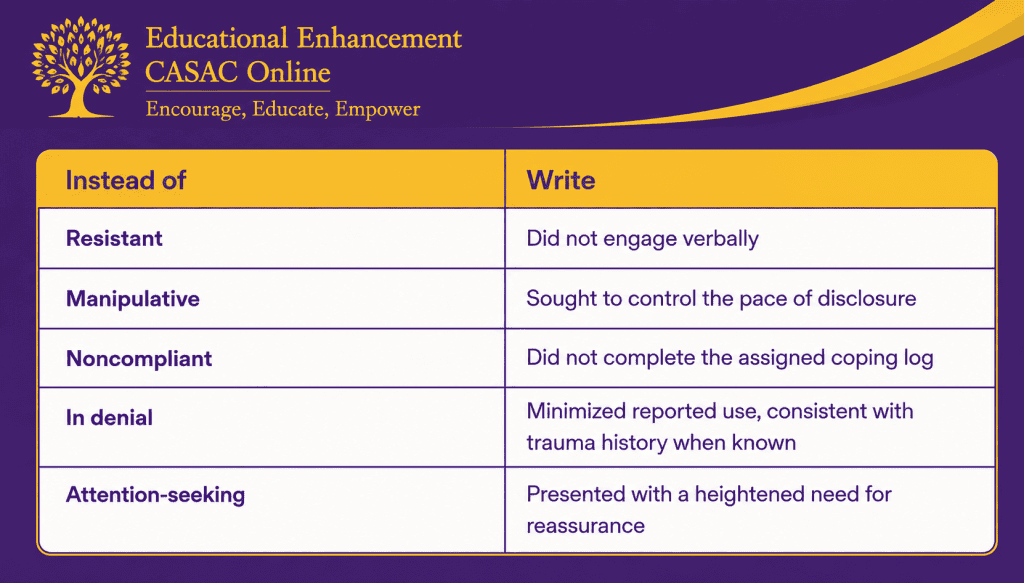
Stigmatizing term → Clinical observation:
Each swap on the right describes behavior. Each term on the left describes a judgment about the person behind it. Trauma-informed progress notes examples almost always come down to this one move: behavior in, motive out.
Four Note Types, Four Examples
Trauma-informed documentation language varies across different notes, reflecting a consistent approach. Here’s how the transition occurs, with examples of trauma-informed progress notes for each type. In all cases, the goal remains: to use language that avoids pathologizing the client’s behavior or disclosures. Ultimately, each assessment hinges on the same question: is this clinical language appropriate for session notes, or is it a judgment cloaked in clinical terms? This focus ensures respectful, supportive, and non-stigmatizing documentation that centers on the client’s experience.
Individual session note. A client raises their voice during a housing conversation and leaves early.
Stigmatizing version: “Client became argumentative and stormed out fifteen minutes early.”
Trauma-informed version: “Client raised their voice discussing housing instability, said the topic felt like too much, and left fifteen minutes early. Plan: revisit at client’s pace next session.”
Group session note. A client stays quiet for the full group.
Stigmatizing version: “Client was withdrawn and resistant to group participation.”
Trauma-informed version: “Client did not speak during group, maintained eye contact with peers, and stayed the full session. Plan: check in individually about comfort level in group.”
Crisis or safety note. A client discloses passive thoughts of suicide.
Stigmatizing version: “Client exaggerates symptoms for attention. Claims of suicidal thoughts seem unlikely given the presentation.”
Trauma-informed version: “Client reported passive suicidal ideation, no plan or intent identified. Safety plan completed collaboratively. Client agreed to contact the crisis line if thoughts intensify.”
This is language that doesn’t pathologize the disclosure itself. It documents risk without turning the client’s honesty into a liability.
Discharge summary. A client transfers to a new program after six months.
Stigmatizing version: Lists diagnosis, attendance, and discharge status with no trauma context at all.
Trauma-informed version: Carries forward a single line of context, something like: “Trust took longer to establish early in treatment, consistent with reported trauma history. Building rapport early supported continued engagement.”
OASAS rules require transferred patients to be treated as continuing in care, with their treatment history carried into the new record. A discharge summary with no trauma context is its own kind of stigmatizing language in documentation: silence where context belongs. It erases continuity before the next provider even opens the chart.
The One-Sentence Test
Before you sign any note, carefully read the last sentence back and ask yourself one crucial question: Does this statement accurately reflect what I actually observed during the session, or is it based on what I assumed or inferred? This step is vital because the clarity and precision of your clinical language in session notes are what ultimately determine whether your documentation holds up under scrutiny or falls apart during review. Accurate, honest descriptions ensure the notes are reliable and useful for ongoing patient care and legal accuracy.
“Client became argumentative” is an assumption about motive. “Client raised their voice” is what happened. The first sentence invites the next reader to judge. The second one just gives them information.
Run the test on:
- Any sentence with a personality label (manipulative, dramatic, difficult)
- Any sentence that explains why, without a direct quote or observed behavior
- Any sentence you wouldn’t want read back to the client
If a sentence assigns motive instead of behavior, rewrite it before you sign it. Passing this test is what produces language that doesn’t pathologize, sentence by sentence. That one habit does more for trauma-informed documentation language than any swap list.
Conclusion
The labels are easy to write. Stigmatizing language in documentation is also expensive, just not in dollars. It costs the client something every time someone new opens the chart. A note is never just a note. It’s a relationship with someone you’ll never meet, conducted on the client’s behalf, ten years before either of you knows it. Trauma-informed progress notes, like the ones above, exist because language that doesn’t pathologize lets that relationship start on the client’s terms, rather than on a label someone wrote in a hurry. Including credentials such as CASAC in NY, CAC, or CADC can further enhance the credibility and trustworthiness of these notes, emphasizing a professional commitment to ethical and compassionate practice.
If you want annotated documentation templates and more trauma-informed progress notes examples built for CASAC charting, Education Enhancement CASAC Online’s course library covers the full framework.
Join Our Newsletter!
Join today. Stay current with news about addiction counselors, interventions, trends, and statistics.
STOP THE STIGMA
